Pediatrics and point‑of‑care MR imaging.
The challenges with conventional imaging in pediatric care.
Before the invention of point-of-care MR imaging, children with acute and chronic neurological conditions had limited options for neuroimaging (ultrasound, CT, and conventional MRI), each with drawbacks.
Ultrasound offers the best point-of-care option and is safe and feasible for newborns because it provides visibility into their brains through the patent anterior fontanelle1. As infants grow, however, their fontanelles close, limiting the clinical utility of cranial ultrasound.

When point-of-care ultrasound is no longer an option, CT and MR assume greater roles in assessing pediatric patients2. Head CTs are often the default imaging modality because they are fast, inexpensive, and readily available to evaluate neurological conditions, especially in the ED setting3. That said, most radiologists and clinicians would prefer to avoid CT and its radiation. Moreover, children with hydrocephalus and ventriculoperitoneal shunts often require serial imaging, and multiple studies have shown that children under the age of nineteen who undergo serial imaging have an increased likelihood of developing brain cancer or leukemia4.
Conventional MRI has been shown to provide better tissue differentiation and visualization of structures over CT5. However, there are challenges that clinicians face when imaging pediatrics with conventional MRI. Factors that contribute to the decision of an MRI over CT include the patient’s ability to tolerate the length of the scan, stability of the patient, and availability of scanners and staff6. Access to a conventional MRI may also be limited due to cost, accessibility, and availability in tertiary care centers that don’t have the staff to run their imaging facilities around the clock.
In 2002, quick brain magnetic resonance imaging (QB-MRI) was introduced for shunt evaluation as an alternative to ionizing radiation exposure from serial imaging with CT and minimizing the need for sedation6. Yue et al. published results of implementing ultrafast spin-echo T2 weighted images on a conventional MRI. They found no statistically significant differences in sensitivity and specificity of QB-MRI versus non-contrast CT6. Twenty years later, head CTs are, unfortunately, the number one scan performed on the pediatric population. According to the American College of Radiology’s Dose Index Registry, which includes 1,543,535 examinations (January 2016–December 2020), 57% of scans were of the head, with 66% of the volume performed in community-based hospitals7.
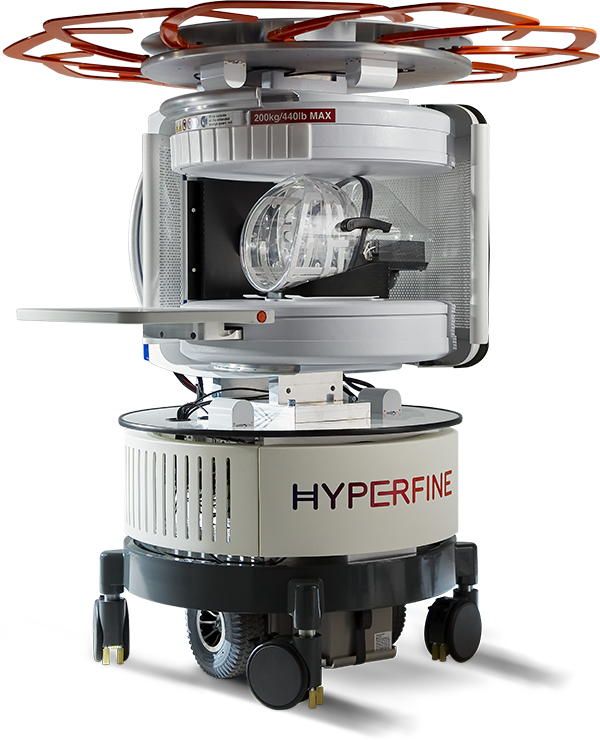
Swoop—the Hyperfine solution.
The Swoop® Portable MR Imaging System™ deploys at the point of care, enabling bedside imaging of children with various clinical conditions. A clinician in a neurosurgery clinic may use the Swoop system to obtain images to check the ventricles of children with suspected hydrocephalus. Alternatively, a pediatric hospitalist may wish to image children with acute conditions in a pediatric intensive care unit. Moreover, in some hospitalized children, the evolution of a child’s condition merits serial imaging, an easy task for the Swoop system. By using the Swoop system, caregivers can track near-real-time changes in condition and recovery—and it accomplishes all of this without subjecting children to ionizing radiation.
The friendly design of the Swoop system is naturally applicable to pediatric brain imaging. The quiet operation, open layout, and built-in safety considerations allow caregivers and family members to be present and comfort a child by holding their hand during the scan.
The benefit of MRI for pediatric hydrocephalus care.
MRI offers a new standard of care for pediatric hydrocephalus patients. In a review of literature by Dopson et al., one 2020 publication reported an 81.1% accuracy of MRI for investigating possible shunt malfunction, which is comparable to CT (82.4%)4.
With the Swoop Portable MR Imaging System™, clinicians can bring the benefits of MRI to a child’s bedside by using Swoop images to help evaluate ventricle size for hydrocephalus follow-up and spare children and staff from ionizing radiation exposure from a CT scan. What’s more, with its Fast T2 sequence, which takes less than three minutes, the Swoop system potentially reduces image deterioration due to movement (and the need to sedate a child for neuroimaging)8.
Swoop system images can help clinicians to diagnose the following neurological conditions:
- Hydrocephalus (diagnosis and monitoring)
- Acute mental status change
- Head injury consequent to a fall or a sports injury
- Leukodystrophy
- Stroke recovery
- Suspected abuse
Swoop in Pediatric Facilities
Learn More
Advanced Image Reconstruction
Deep Learning Image Reconstruction
1. Ichihashi K, Nonaka K. Point-of-care ultrasound for children. Journal of Medical Ultrasonics. Published online January 21, 2022. doi:10.1007/s10396-021-01169-0
2. Tekes, A., Jackson, E. M., Ogborn, J., Liang, S., Bledsoe, M., Durand, D. J., Jallo, G., & Huisman, T. A. G. M. (2016). How to Reduce Head CT Orders in Children with Hydrocephalus Using the Lean Six Sigma Methodology: Experience at a Major Quaternary Care Academic Children’s Center. American Journal of Neuroradiology, 37(6), 990–996. doi.org/10.3174/ajnr.a4658
3. Ramgopal, S., Karim, S. A., Subramanian, S., Furtado, A. D., & Marin, J. R. (2020). Rapid brain MRI protocols reduce head computerized tomography use in the pediatric emergency department. BMC Pediatrics, 20(1). doi.org/10.1186/s12887-020-1919-3
4. Dopson G., Dalton A., Nicholson C., Jenkins A., Mitchell P., Cowie C. (2020) CT scan exposure in children with ventriculoperitoneal shunts: single-center experience and review of the literature. Child’s Nervous System. 36:591-599. doi.org/10.1007 /s00381-019-04345-3
5. Themes UFO. Magnetic Resonance Imaging in the Pediatric Patient. Radiology Key. Published August 20, 2019. https://radiologykey.com/magnetic-resonance-imaging-in-the-pediatric-patient/
6. Yue, E., et al., Test characteristics of quickbrain MRI for shunt evaluation in children: an alternative modality to avod radiation. J Neurosurg Pediatr (2015) 15:420-426. https://doi.org/10.3171/2014.9.PEDS14207
7. Kanal, K., et al.. U.S. Diagnostic Reference Levels and Achievable Doses for 10 Pediatric CT Examinations. Radiology (2021) 000:1-11. https://doi.org/10.1148/radiol.2021211241
8. Barkovich, M. J., Xu, D., Desikan, R. S., Williams, C., & Barkovich, A. J. (2018). Pediatric neuro MRI: tricks to minimize sedation. Pediatric radiology, 48(1), 50–55. https://doi.org/10.1007/s00247-017-3785-1
Big tech in a small package.
The Hyperfine Swoop system is the only portable MRI that can move to your patient's bedside at the point of care, plug into a standard electrical outlet, and acquire critical neuroimages within minutes. No waiting. No patient transport.